


Description
Buy O-DSMT Powder UK Online | O-DSMT Powder For Sale UK
DESCRIPTION
Buy O-DSMT (O-desmethyltramadol , Omnitram)
Buy O-DSMT Powder UK Online. In the expanding world of research chemicals and novel synthetic compounds, O-DSMT (O-Desmethyltramadol) has emerged as a substance of significant interest. Unlike many obscure research chemicals with little pharmacological history, O-DSMT is actually the primary active metabolite of the prescription analgesic tramadol. This distinction gives it a more documented pharmacological profile than most novel synthetic opioids, yet its emergence as a standalone research chemical and recreational substance has raised serious concerns among harm reduction specialists and medical professionals alike.
This comprehensive guide examines O-DSMT powder from multiple angles: its chemical structure and physical appearance, its mechanism of action, potential uses (research only), essential safety protocols, and withdrawal management strategies. All information is provided for educational and harm-reduction purposes only. O-DSMT is not approved for human consumption in any country as of 2025, and its use carries significant risks including addiction, respiratory depression, and death.
O-DSMT powder occupies an unusual position in the landscape of novel synthetic drugs: it is simultaneously a well-characterized pharmaceutical metabolite with legitimate research applications and a dangerous unregulated opioid responsible for documented overdose deaths.
Its pharmacology as a μ-opioid receptor agonist with additional norepinephrine reuptake inhibition gives it a unique profile—more predictable than tramadol, more stimulating than classical opioids, but still carrying the same core risks: addiction, respiratory depression, and fatal overdose. The tragic “Krypton” deaths in Sweden serve as an undeniable reminder that O-DSMT is not a safe alternative to traditional opioids.
If you are a researcher handling this compound, use appropriate laboratory safety protocols and understand its potency. If you or someone you know is using O-DSMT recreationally, prioritize harm reduction: accurate milligram dosing, never using alone, having naloxone available, and recognizing that withdrawal may require medical support. Opioid dependence is treatable, and help is available through addiction medicine specialists, detoxification programs, and mental health services.
- MW: 249.354 g/mol
- IUPAC: 3-[2-[(dimethylamino)methyl]-1-hydroxycyclohexyl]phenol
- Usage: Stimulant
- Name: O-Desmethyltramadol
- MF: C15H23NO2
What Is O-DSMT? Understanding the Chemistry
O-DSMT stands for O-Desmethyltramadol, also known by its International Nonproprietary Name (INN) desmetramadol. It belongs to the phenylpropylamine class of compounds and is structurally related to the prescription opioid tramadol.
Molecular Details
-
Chemical Formula: C₁₅H₂₃NO₂
-
Molecular Weight: 249.354 g/mol
-
IUPAC Name: 3-[(1R,2R)-2-[(dimethylamino)methyl]-1-hydroxycyclohexyl]phenol
-
CAS Registry Number: 144830-14-8
-
SMILES: CN(C)C[C@H]1CCCC[C@]1(O)C1=CC(O)=CC=C1
The Tramadol Connection
To understand O-DSMT, one must understand tramadol. Tramadol is a prodrug—it requires metabolism by the liver enzyme CYP2D6 to convert it into its active form, O-DSMT. This explains why tramadol’s effects vary significantly between individuals: “poor metabolizers” (those with less active CYP2D6) experience reduced pain relief, while “ultra-rapid metabolizers” may experience enhanced effects and increased toxicity risk.
O-DSMT itself requires no metabolism to produce its analgesic effects. This makes it pharmacologically distinct from tramadol and bypasses the genetic variability issues associated with its parent compound.
Pharmacodynamics: How It Works
O-DSMT is primarily a μ-opioid receptor (MOR) full agonist. This is the same primary mechanism as classic opioids like morphine, oxycodone, and heroin. Key pharmacological features include:
-
G-protein biased agonism at the μ-opioid receptor, which in preclinical studies suggests potentially reduced respiratory depression compared to classical opioids
-
Norepinephrine reuptake inhibition (primarily from the (-)-enantiomer), contributing to stimulant-like effects at lower doses
-
5-HT2C receptor antagonism, which may contribute to antidepressant properties
-
Negligible serotonin reuptake inhibition—unlike tramadol, which has significant serotonin activity
The combination of opioid agonism and norepinephrine reuptake inhibition creates what users describe as a more “functional” or “stimulating” opioid effect compared to classical opioids like morphine or heroin.
Pharmacokinetics
-
Half-life: 6-8 hours
-
Metabolism: Primarily via CYP3A4 and CYP2B6 into N,O-didesmethyltramadol
-
Duration of effects: 6-10 hours depending on route of administration
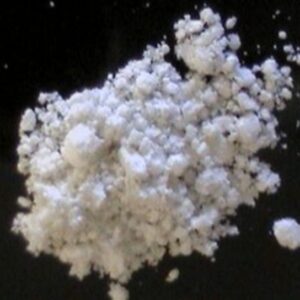
Physical Appearance of O-DSMT Powder
Based on analytical laboratory reports and user descriptions, O-DSMT powder typically presents with the following physical characteristics:
-
Color: White to off-white
-
Texture: Described as “grainy” or having a “salt-like” texture
-
Form: Crystalline powder
-
Solubility: Not extensively documented, but as a hydrochloride salt (common form), it is typically soluble in water and alcohol
A laboratory analysis by DrugsData.org (formerly EcstasyData) of a sample sourced from China in 2022 confirmed these characteristics: a white powder with a “grainy/salt texture”.
Purported Uses and Applications
O-DSMT has several contexts of use, ranging from legitimate research to recreational consumption.
1. Analytical and Pharmacological Research
As the active metabolite of a widely prescribed medication, O-DSMT serves as an important analytical reference standard for:
-
Forensic toxicology (identifying tramadol use via metabolite detection)
-
Pharmacokinetic studies
-
Structure-activity relationship research for novel analgesics
2. Clinical Investigation (Discontinued)
O-DSMT was investigated clinically under the name Omnitram as a potential novel analgesic. Human trials suggested it offers analgesic benefits comparable to oxycodone and fentanyl but with potentially reduced respiratory depression and a comparatively favorable safety profile. However, clinical development appears to have stalled, and as of 2025, O-DSMT is not approved for medicinal use in any country.
3. Recreational Use
Despite its lack of medical approval, O-DSMT has appeared on the recreational drug market, typically as:
-
A white powder sold through online research chemical vendors
-
An adulterant in other products (most notably the “Krypton” herbal blend containing kratom leaf powder laced with O-DSMT)
Users report effects including:
-
Sedation and relaxation (at higher doses)
-
Euphoria
-
Pain relief
-
Anxiety suppression
-
Mild stimulation (at lower doses, due to norepinephrine reuptake inhibition)
Unlike tramadol, which many users find stimulating, O-DSMT is described as feeling “considerably closer to a traditional opiate”.
where to order O-DSMT powder near me europe | buy O-DSMT powder germany | buy research chemicals online sweden
Benefits (Theoretical and Research-Based)
It is critical to emphasize that O-DSMT has no approved medical use and is not safe for unsupervised human consumption. However, research has identified several theoretical benefits that drove clinical development interest:
1. Reduced Respiratory Depression Risk
Preclinical and early clinical data suggest that O-DSMT’s G-protein biased signaling at the μ-opioid receptor may produce analgesia with less respiratory depression than classical opioids like fentanyl or morphine. This is potentially significant, as respiratory depression is the primary cause of fatal opioid overdose.
2. Genetic Predictability
Unlike tramadol, whose effects vary widely based on CYP2D6 genotype, O-DSMT’s effects are consistent across different individuals’ metabolic capacities. This makes it theoretically more reliable as an analgesic.
3. Dual Mechanism for Pain Management
The combination of μ-opioid agonism and norepinephrine reuptake inhibition may provide advantages for neuropathic pain and complex pain syndromes where pure opioids are less effective.
4. Potential Antidepressant Properties
O-DSMT is a 5-HT2C receptor antagonist. Antagonism of this receptor is associated with increased dopamine and norepinephrine release in the prefrontal cortex and is a mechanism shared by some antidepressants. This may explain why some tramadol users report mood-elevating effects beyond simple opioid euphoria.
5. Lower Seizure Risk Compared to Tramadol
Tramadol is known to lower seizure threshold, primarily through its serotonin and norepinephrine reuptake inhibition. O-DSMT lacks significant serotonin activity and may therefore have a lower seizure risk.
Addiction and Dependence
O-DSMT is considered moderately to highly addictive with significant abuse potential. Regular use leads to:
-
Tolerance (requiring larger doses for the same effect)
-
Physical dependence (withdrawal symptoms upon cessation)
-
Psychological dependence (cravings and compulsive use)
Dangerous Drug Interactions
Combining O-DSMT with other central nervous system depressants is potentially fatal:
-
Alcohol – Increased respiratory depression
-
Benzodiazepines (Xanax, Valium, etc.) – Synergistic depression
-
Other opioids – Additive effects
-
Gabapentinoids – Enhanced sedation and respiratory risk
Safe Usage Tips (Harm Reduction)
If O-DSMT is being used despite warnings, the following harm-reduction practices are essential to minimize risk of death.
1. Accurate Dosing Is Critical
O-DSMT is potent and dosing varies significantly by route of administration. The following dosage ranges are compiled from user reports and should be considered estimates only—individual sensitivity varies dramatically:
Oral Administration (most common, safer than other routes):
-
Threshold: 5 mg
-
Light dose: 10-25 mg
-
Common dose: 25-50 mg
-
Strong dose: 50-100 mg
-
Heavy dose: 100+ mg
Sublingual Administration:
-
Threshold: 5 mg
-
Light dose: 10-25 mg
-
Common dose: 25-50 mg
-
Strong dose: 50-80 mg
-
Heavy dose: 80+ mg
Intravenous Administration (highest risk):
-
Threshold: 5 mg
-
Light dose: 5-12.5 mg
-
Common dose: 12.5-25 mg
-
Strong dose: 25-50 mg
-
Heavy dose: 50+ mg
2. Always Use a Milligram Scale
Never estimate doses visually—powder density varies dramatically between batches. A milligram scale (0.001g accuracy) is non-negotiable.
3. Start Low, Go Slow
If you have no opioid tolerance, start at or below the threshold dose (5 mg or less). Wait at least 2 hours before considering redosing, as peak effects may take 2-5 hours to manifest orally.
4. Route of Administration Considerations
-
Oral is the safest and most predictable route. Effects last 6-10 hours with onset in 20-40 minutes.
-
Sublingual offers faster onset but similar duration.
-
Intravenous produces effects within seconds but dramatically increases overdose risk and should be avoided entirely.
-
Intranasal (snorting) is not well-documented for O-DSMT and may have unpredictable absorption.
5. Do Not Mix
Avoid combining O-DSMT with:
-
Alcohol – Potentially fatal respiratory depression
-
Benzodiazepines – Synergistic depression
-
Other opioids or depressants
-
Stimulants – Masks sedation, leading to accidental overdose
6. Never Use Alone
If use occurs, ensure someone is present who can recognize overdose symptoms (slow breathing, unresponsiveness, blue/gray lips or fingertips) and administer naloxone (Narcan) if available. Naloxone is an opioid antagonist that can temporarily reverse opioid overdose—but multiple doses may be required for potent synthetic opioids.
7. Recognize the “Norepinephrine Ceiling”
Long-term users report that O-DSMT’s norepinephrine reuptake inhibition creates a “ceiling effect” —as tolerance to the opioid effects builds, the stimulating/adrenergic side effects become
more prominent, leading to unpleasant experiences including jitteriness, anxiety, and crash states. This often signals that tolerance has reached a point where continued use will produce diminishing returns with increasing side effects.
Withdrawal and Discontinuation Tips
O-DSMT produces physical dependence with regular use. Withdrawal symptoms typically begin 12-24 hours after the last dose and peak around days 2-3.
Common Withdrawal Symptoms
Based on user reports and opioid withdrawal literature:
Physical symptoms:
-
Muscle aches and bone pain
-
Sweating and chills
-
Runny nose and watery eyes
-
Nausea, vomiting, diarrhea
-
Dilated pupils
-
Yawning and fatigue
-
Insomnia or restless sleep
Psychological symptoms:
-
Anxiety and agitation
-
Depression and anhedonia (inability to feel pleasure)
-
Intense drug cravings
-
Irritability
-
Difficulty concentrating
Withdrawal Timeline
For O-DSMT specifically (half-life 6-8 hours):
-
Onset: 12-24 hours after last dose
-
Peak severity: Days 2-3
-
Physical symptoms subside: Days 5-7
-
Post-acute withdrawal (PAWS) : Weeks to months for some individuals (mood disturbances, sleep issues, cravings)
A user reporting after 2 weeks of daily use noted withdrawal symptoms lasting “less than a week” with physical symptoms resolving in about 2 days. However, longer-term or higher-dose use produces more severe and prolonged withdrawal.
Tips for Managing Withdrawal
Tapering (reducing dose gradually) is strongly preferred over abrupt cessation (“cold turkey”):
-
Taper protocol: Reduce dose by 10-20% every 2-3 days. For example, from 50 mg/day → 40 mg → 32 mg → 25 mg, etc.
-
Switch to oral route if using other routes—oral provides smoother blood levels for tapering.
-
Over-the-counter symptomatic relief:
-
Loperamide (Imodium) for diarrhea
-
Ibuprofen or acetaminophen for muscle aches
-
Antihistamines (diphenhydramine/Benadryl) for sleep—use cautiously as they may worsen restless legs
-
Magnesium supplements for muscle cramps
-
-
Prescription options (if available through medical provider):
-
Clonidine (reduces autonomic symptoms like sweating, racing heart)
-
Gabapentin or pregabalin (for anxiety and restless legs)
-
Zofran (ondansetron) for nausea
-
-
Hydration and nutrition – Withdrawal often causes fluid loss from diarrhea and sweating. Electrolyte solutions (Pedialyte, sports drinks) are helpful.
-
Avoid antihistamines with restless legs – Many users report that diphenhydramine (Benadryl) worsens the characteristic opioid withdrawal symptom of restless legs and should be avoided.
When to Seek Professional Help
Medical detoxification is recommended for:
-
Inability to stop despite multiple attempts
-
Severe withdrawal symptoms (vomiting, diarrhea leading to dehydration)
-
Suicidal thoughts or severe depression
-
History of seizures or other medical conditions
-
Polysubstance dependence (especially alcohol or benzodiazepines)
Long-Term Recovery
Opioid dependence is a chronic condition. After acute withdrawal:
-
Consider naltrexone (opioid antagonist) to prevent relapse—available as daily pill or monthly injection
-
Seek counseling or support groups (SMART Recovery, peer support)
-
Address underlying pain or mental health conditions that may have contributed to use
As of 2025, O-DSMT is not approved for medical use in any country. Its sale is typically restricted to research purposes only, though it continues to appear on the recreational market.
O-DSMT powder occupies an unusual position in the landscape of novel synthetic drugs: it is simultaneously a well-characterized pharmaceutical metabolite with legitimate research applications and a dangerous unregulated opioid responsible for documented overdose deaths.
Its pharmacology as a μ-opioid receptor agonist with additional norepinephrine reuptake inhibition gives it a unique profile—more predictable than tramadol, more stimulating than classical opioids, but still carrying the same core risks: addiction, respiratory depression, and fatal overdose. The tragic “Krypton” deaths in Sweden serve as an undeniable reminder that O-DSMT is not a safe alternative to traditional opioids.
If you are a researcher handling this compound, use appropriate laboratory safety protocols and understand its potency. If you or someone you know is using O-DSMT recreationally, prioritize harm reduction: accurate milligram dosing, never using alone, having naloxone available, and recognizing that withdrawal may require medical support. Opioid dependence is treatable, and help is available through addiction medicine specialists, detoxification programs, and mental health services.